Originally published in AARP’s Health Medicare Resource Center By Dena Bunis, AARP, March 2018
Medicare is asking doctors to play a new video in their waiting rooms to remind patients that the federal government will begin mailing them new identification cards next month.
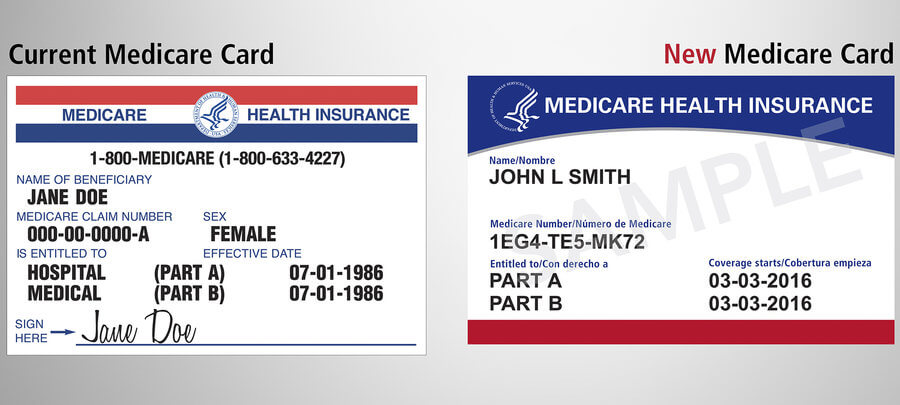
The video gives beneficiaries a glimpse at what the new card will look like and explains why and how it was modified. Instead of a Social Security number, the cards will display an 11-digit Medicare beneficiary identifier, and they will no longer include gender and a signature.
Eliminating the personal details, Centers for Medicare and Medicaid Services (CMS) officials say, will better protect an enrollee’s identity and guard against fraud.
The Social Security Administration (SSA) urges Medicare enrollees to make sure the agency has their correct address on file. You can go to socialsecurity.gov/myaccount or call 800-772-1213 to update your address.
Scammers with various ploys have already started to target the 58 million individuals who will be getting new cards. The Federal Trade Commission (FTC) reports that con artists are calling beneficiaries and pretending to be from Medicare, then trying to talk them into paying for the revised card. Medicare will never call and ask for any personal identification or money for the new cards. The cards are free and will be mailed to members’ homes.
Medicare beneficiaries in Delaware, the District of Columbia, Maryland, Pennsylvania, Virginia and West Virginia will be the first enrollees to receive the replacement cards. The mailings will continue through 2019.
Author: Lois A. Bowers, Senior Editor, McKnight’s Senior Living
Family support is the biggest influencer of housing and care preferences among older adults, according to a study published Wednesday (March 7, 2018) in the Journal of the American Geriatrics Society.
Often, the authors found, older adults changed their preferences based on the concerns of family members or a wish to avoid “being a burden” to others. This basis was especially true for preferences regarding the places where people wished to receive care — for example, at home or in a residential care setting, they said.
The researchers, all of whom were affiliated with the Cicely Saunders Institute of Palliative Care Policy and Rehabilitation at Kings College London, examined 57 previous studies about the preferences of older adults with advanced illness. They included research that investigated preferences for where people wanted to be cared for, the kinds of communication and decision-making they wanted and the quality of life they hoped to have over time.
Family involvement is key in care decisions
Although support from family was the most important influence on their care preferences, older adults usually formed their preferences based on several other factors, too, including their experiences related to previous illness and caring for others as well as having a serious illness, according to the study.
In this post, a physician connects his personal and professional caregiver roles.
As palliative care providers, we spend our careers talking about end-of-life care and helping families make difficult choices about life and death. Have you ever been on the other side of the conversation, answering questions and making decisions for your own loved ones? I have cared for thousands of patients at the end of life, but recently I’ve been on the other side of that conversation – twice.
My first conversation began with “Momma,” my wife’s 91-year-old paternal grandmother. Her decline started with a kidney stone, which then led to urinary tract infections and tremendous pain. Momma made the decision to have lithotripsy. During the procedure, she had respiratory distress and required intubation. Her heart was not strong enough to tolerate this “routine” procedure. She developed right-sided heart failure and pulmonary edema. Doctors were able to extubate her; however, she continued to have more respiratory distress. She was not doing well. They placed her on Bi-pap but she did not tolerate this. She was in the hospital, agitated, dyspneic, and did not want to be re-intubated.
So now what? Our family had to begin those difficult discussions. Do we continue to push aggressive care? Momma told the family she was tired and ready to die. It was hard for our family to acknowledge what this meant even knowing her wishes. Added to that, it was two weeks before Christmas and my family lived six hours away from Momma. We decided my wife and our three-year-old daughter would travel to Georgia while I stayed home to work. I wanted my wife to be there for the conversation in person and to see her grandmother, as I knew this might be her final days on earth. After discussing options, the family agreed to inpatient hospice care.
I was too involved with work and like many times before chose work over family. My wife was at Momma’s bedside for less than 24 hours when she called me telling me that Momma was asking for me, “The Doctor.” I pulled myself away from work in the middle of the day and headed to Georgia.
I was now being asked medical questions as well as “what about Christmas?”, “what do we tell the great-grandchildren?”, and “is this the right thing to do?” I did not have answers. I had memories and emotions for this woman I loved; I did not want to think, “Momma is dying.”
All the signs were there; it was her time to die. The family began the journey with Momma. I have worked in three different inpatient hospice facilities. It’s easier for me to study the staff, their workflow, their EMR, their census, their medical director – this is what I know. My wife reminded me that this time, I was there for Momma and our family. I was not “The Doctor” now; I was family.
Staff managed Momma’s symptoms quickly and she had two good days talking and interacting. We had made the right choice, albeit not an easy one. Long days and nights at the hospice home wear a family down. Hospice staff participate in these experiences daily. We think how hard it must be for the patients and families. When you are on the other side, you feel the sorrow and you learn a lot about the value of hospice care.
Momma died peacefully four days later. We returned home to North Carolina, only to receive a phone call that “Granny” was in the hospital. Granny was my wife’s 78-year-old maternal grandmother. She had Alzheimer’s disease, had fallen at home, and had developed altered mental status. She was not eating, she had a UTI, and a CT scan showed a small hemorrhage in the frontal lobe. Granny was agitated, not eating, and declining. So now what?
Just three weeks earlier we had lost Momma. Now our family was deciding on inpatient hospice for Granny.
My wife, daughter, and I packed the car and headed for Florida. I took the time from work, but I was still on call and was on the phone, giving orders the entire trip. Once again, it was easier for me to do my work as a hospice physician than confront what I had no control over. We were losing both our grandmothers within three weeks.
As we arrived in the middle of the night, we received a call letting us know Granny died. She had declined quickly. That was truly a blessing. After all the heartbreak and tears, we went to Granny’s house and celebrated her life. This is what she would have wanted.
Those two experiences remind me how hard end-of-life conversations are for families. We as palliative care providers need to remember it is different when there are memories and emotions involved. No matter how informed our families are, these decisions are not easy. And, it’s hard being on the other side. We are no longer medical professionals, we are family. All our medical training leaves our mind and we become an emotional basket case. We find it hard to think straight or make rational decisions. It’s difficult living with the decisions and through those choices.
I’m 40 years old, my parents are approaching retirement, and my grandparents are dying. I have friends who are struggling with acute and chronic illnesses. All of this has made me a better hospice and palliative care physician and I’m glad I can reflect on my training and life experiences to help my patients and families. I make the conversations personal and emotional. I have more empathy during family meetings. I think this adds a new dimension to the work I do, the work I’m proud to do.
These two experiences brought our family closer together and I’m grateful I could help in the decision-making process. My family saw firsthand how our jobs as hospice and palliative care providers are intensely emotional. We all need to realize the impact we have on the families we care for, how a well-trained hospice and palliative care staff can have an impact on a family.
During our trip home from Florida, my wife looked at me and asked, “How do you do this day after day? I am proud of you and now understand your job even more and how rewarding it must be.”
———–
Christopher M. Thompson, MD, HMDC, assisted in developing the palliative medicine programs at two hospitals prior to joining Transitions LifeCare as Medical Director for Transitions Kids, Transitions LifeCare’s pediatric hospice program. Dr. Thompson is board certified in Family Medicine. After completing his Fellowship, Dr. Thompson became board certified in Hospice and Palliative Medicine with the added qualification of Hospice Medical Director Certification.
Professionals who care. Helping improve people’s lives is at the heart of social work
In honor of National Social Work Month in March, below are facts about social workers from the National Association of Social Workers:
About Social Workers
Social workers seek to improve the lives of others.
Social work is a profession for those with a strong desire to help improve people’s lives. Social workers assist people by helping them cope with issues in their everyday lives, deal with their relationships, and solve personal and family problems.
According to the Bureau of Labor Statistics, there were almost 650,000 social workers in the United States in 2014. With an expected growth in jobs of 12 percent by 2024, social work is one of the fastest growing professions in the United States.
Who are social workers?
Social work is a profession for those with a strong desire to help improve people’s lives. Social workers assist people by helping them cope with issues in their everyday lives, deal with their relationships, and solve personal and family problems.
Some social workers help clients who face a disability or a life-threatening disease or a social problem, such as inadequate housing, unemployment, or substance abuse. Social workers also assist families that have serious domestic conflicts, sometimes involving child or spousal abuse.
Some social workers conduct research, advocate for improved services, engage in systems design or are involved in planning or policy development. Many social workers specialize in serving a particular population or working in a specific setting.
What do social workers do?
Social workers help individuals, families, and groups restore or enhance their capacity for social functioning, and work to create societal conditions that support communities in need.
The practice of social work requires knowledge of human development and behavior, of social, economic and cultural institutions, and of the interaction of all these factors.
Social workers help people of all backgrounds address their own needs through psychosocial services and advocacy.
Social workers help people overcome some of life’s most difficult challenges: poverty, discrimination, abuse, addiction, physical illness, divorce, loss, unemployment, educational problems, disability, and mental illness. They help prevent crises and counsel individuals, families, and communities to cope more effectively with the stresses of everyday life.
Who employs social workers?
Professional social workers are found in every facet of community life—in schools, hospitals, mental health clinics, senior centers, elected office, private practices, prisons, military, corporations, and in numerous public and private agencies that serve individuals and families in need. Many also serve as social and community service directors.
According to the Substance Abuse and Mental Health Services Administration (SAMHSA), professional social workers are the nation’s largest group of mental health services providers. There are more clinically trained social workers—over 200,000—than psychiatrists, psychologists, and psychiatric nurses combined. Federal law and the National Institutes of Health recognize social work as one of five core mental health professions.
The S. Department of Veterans Affairsemploys more than 13,000 professional social workers. It is one of the largest employers of MSWs in the United States.
More than 40% of all disaster mental health volunteers trained by the American Red Cross are professional social workers.
There are hundreds of social workers in national,state and local elected office,These include one U.S. Senator and six U.S. Representatives. Sen. Debbie Stabenow (MI), Rep. Barbara Lee (CA-13), Rep. Kyrsten Sinema (AZ-9), Rep. Carol Shea-Porter (NH-1), Rep. Luis Gutierrez (IL-4), Rep. Niki Tsongas (MA-3) and Rep. Susan Davis (CA-53).
Today, almost 50 special interest organizations contribute to the vitality and influence of the social work profession. There are social work groups for educators and researchers, as well as organizations for practitioners in health care leadership, nephrology, oncology, child welfare, schools, prisons, courts, and many other settings.
The single best way to prevent seasonal flu is to get vaccinated each year, but good health habits like covering your cough and washing your hands often can help stop the spread of germs and prevent respiratory illnesses like the flu. There also are flu antiviral drugs that can be used to treat and prevent flu.
Avoid close contact.
Avoid close contact with people who are sick. When you are sick, keep your distance from others to protect them from getting sick too.
Stay home when you are sick.
If possible, stay home from work, school, and errands when you are sick. This will help prevent spreading your illness to others.
Cover your mouth and nose.
Cover your mouth and nose with a tissue when coughing or sneezing. It may prevent those around you from getting sick.
Clean your hands.
Washing your hands often will help protect you from germs. If soap and water are not available, use an alcohol-based hand rub.
Avoid touching your eyes, nose or mouth.
Germs are often spread when a person touches something that is contaminated with germs and then touches his or her eyes, nose, or mouth.
Practice other good health habits.
Clean and disinfect frequently touched surfaces at home, work or school, especially when someone is ill. Get plenty of sleep, be physically active, manage your stress, drink plenty of fluids, and eat nutritious food.
A nurse.com article by Sallie Jimenez focused on item #4 and shared a study concluding that hand washing decreases chances for the illness to result in deaths. Jimenez writes that “In the midst of what may be one of the worst flu outbreaks in a decade, new research reinforces the importance of proper hand hygiene protocol.”
Her article references the following: A study published in the February issue of the American Journal for Infection Control found hand washing saves lives — not just in hospitals — but all healthcare facilities, including nursing homes. Researchers looked at 26 French nursing homes from April 1, 2014, to April 1, 2015, discovering consistent measures encouraging staff and visitors to wash their hands reduces mortality and antibiotic prescription rates, according to a news release from the Association for Professionals in Infection Control and Epidemiology highlighting the results.
During the course of the study, which included 13 nursing homes randomly assigned to an intervention group and 13 assigned to a control group, a program was implemented targeting nursing home staff, visitors and outside care providers, the news release said.
As part of the program, hand sanitizer became more readily available in both pocket-sized containers and dispensers and the idea of proper hand hygiene was promoted through posters, events, work groups and education.
“The measures resulted in a lower mortality rate of 2.10 deaths per 100 residents, versus 2.65 in the control group, with a notable 30% decrease in the mortality rate during France’s major influenza outbreak in early 2015, according to the news release.”
Although the CDC stresses the single best way to prevent the flu is to get vaccinated, proper hand washing and cleansing — either with soap and water or an alcohol-based hand sanitizer if soap and water are not available — also is recommended.
Last week was tough. The world witnessed a tragedy that has become all too familiar, another school shooting. A day that was supposed to be about love and peace, turned dark and cold for so many. On the day after, when I dropped my little dude, Jason, off at his school, he dashed into his classroom shoving his backpack into his cubby, and my heart just broke into pieces for the families of the victims in Parkland, FL.
How could one person take seventeen beautiful souls, most of them being children? We ask ourselves why did this have to happen, we say prayers for the families who now have to learn how to move on without their child, and we call on congress for change, yet again. It’s hard to imagine how you go on after such a devastating tragedy. Simple things like going back to work, seem like mountains to climb. While we look for answers, one thing is for sure; time doesn’t stand still for the ones who need it to the most. Instead, you learn how to compromise with time, and make the most of what he gives you. We find ourselves pleading for time to just stand still, to have just five more minutes with the ones we love. But you see, time doesn’t wait for no one, and this is why there is more to life than the nine-to-five grind.
We find our humanity—our will to live and our ability to love—in our connections to one another.― Sheryl Sandberg, Option B: Facing Adversity, Building Resilience, and Finding Joy
As I mentioned at the beginning of this post, last week was tough. Sometimes you don’t get a “do over”. What you do get is a chance to put things in perspective, and not take the life you’ve been blessed with for granted. So on a whim, my husband, Travis, says to me, “you know, we can take a road trip, South, and hang out with your parents”. So, we took advantage of the long weekend (President’s Day), loaded up the truck, and off we went! And as you can imagine with a nine hour drive, I had time to reflect, time to think, and time to write…
All this time got me thinking, how can employers and HR support employees through grief and loss? Are bereavement leave policies enough? I started to research this and one article from SHRM stood out. Click here to read more. In a time of unspeakable loss, what are some big things that HR can do to support their employees and organization?
1) It’s more than policy – It’s about having a plan:
To my fellow HR professionals, let’s work together with management and executives to create a plan to support employees in their time of need. We should do more than just contact the employee and share information about our organization’s bereavement policy. One great example is what Ernst & Young did last year. They provided dedicated HR support to the family of one of their employees who was critically hurt in the Las Vegas mass shooting tragedy. Thankfully, this EY employee survived, and her story showed us that having a plan can lessen the burden on the employee and her family. It shows us that an employer can really champion for their employees when they need us to the most.
2) It’s time to lead the way:
What can we do to prepare fellow employees for a grieving employee’s return to work? There are a lot of emotions that the employee will still be dealing with upon his return. There will be lack of focus, and difficulty with concentrating, even on the simplest of tasks. We as HR professionals have to partner with management on creating a smooth path for the grieving employee as they return to the workplace. We need to lead the way in helping the grieving employee navigate back into the environment. It is vital for his success.
3) Give some space – It takes time:
I think the single most important thing we can do to help a grieving employee return to work is to give space. What if we created a private place where the grieving employee can go to take a break when she is feeling overwhelmed with emotions? These emotions will come in waves and it is important to give space.
Some “Chelles” find their way to shore, while some live in the sea for eternity. ― Michelle Kohlhof
My closing thought, take the time to set eyes on the ones you love, and are blessed to still have in your life. It’s another chance to fill your pocket full of “Chelles”.
For centuries, journaling has been a tool for self-discovery. With reflective writing, your words do not have to be carefully arranged. It’s your private world and your private thoughts. You can ramble. Mention the unthinkable. Explore ideas with no worry about the consequences.
Writing as personal therapy
Journaling can help us turn a jumbled set of feelings into a coherent story. It can give us a better sense of ourselves as the author of our lives rather than a victim of circumstances. Research on writing as “expressive therapy” has revealed that it can:
Increase happiness
Reduce symptoms of anxiety and depression
Strengthen the immune system, especially for those coping with physical or medical challenges
Some guidance
You or your loved one may wish to try journaling. Great! A few caveats. Studies have shown:
If you’re dealing with a major depression or other significant mental health challenge, journal in conjunction with a therapist.
If you recently experienced a significant trauma, wait a few months. Writing too soon, when emotions are raw, may make you feel worse.
It is possible to get mired in the negative. Write about your worries and concerns, but don’t just vent. Look for a meaning or purpose behind your thoughts.
Writing that is solution-oriented provides greater benefit. Exploring strategies to address problems and acknowledging the positives of a situation are important components to making a journaling session therapeutic.
How to get the most out of journaling
Pick a quiet, private place where you can write without interruption.
Write continuously for 20 minutes about whatever comes to mind. (Aim to do this daily for four days in a row.)
Don’t worry about spelling or grammar. This writing is for your eyes only.
Prioritize issues.
Track your triggers and responses. Look for patterns.
Talking to Doctors About Your Bucket List Could Help Advance Care Planning
February 8, 2018 by Stanford University Medical Center
For physicians, asking patients about their bucket lists, or whether they have one, can encourage discussion about making their medical care fit their life plans, according to a study by researchers at the Stanford University School of Medicine.
A bucket list is a list of things you’d like to do before you die, like visiting Paris or running a marathon. It’s a chance to think about the future and put lifelong dreams or long-term goals down on a piece of paper.
For doctors, knowing their patients‘ bucket lists is a great way to provide personalized care and get them to adopt healthy behaviors, said VJ Periyakoil, MD, clinical associate professor of medicine, who said she that she routinely asks her patients if they have a bucket list.
“Telling a patient not to eat sugar because it’s bad for them doesn’t work nearly as well as saying, for example, if you are careful now, you will be able to splurge on a slice of wedding cake in a few months when your son gets married,” Periyakoil said.
The study will be published Feb. 8 in the Journal of Palliative Medicine. Periyakoil, an expert in geriatrics and palliative care, is lead author.
The researchers, who surveyed 3,056 participants across the United States, found that by far the majority of respondents—91 percent—had made a bucket list. Survey results also showed that respondents who reported that faith and spirituality were important to them were more likely to have made a bucket list. The older the respondents were, the more likely they were to have a bucket list, and, not surprisingly, those younger than 26 tended to include more “crazy things” on their lists, such as skydiving.
Bucket list categories
Six general themes tended to describe the items on respondents’ bucket lists: 79 percent included travel; 78 percent included accomplishing a personal goal, such as running a marathon; 51 percent included achieving a life milestone, such as a 50th wedding anniversary; 16.7 percent included spending quality time with friends and family; 24 percent included achieving financial stability; and 15 percent included a daring activity.
“When you just Google the term ‘bucket list,’ it’s huge how much interest there is in this,” Periyakoil said. “It provides a very nice framework for thinking about your life goals, health and your mortality.”
Past research has found that when doctors talk to patients—especially those with chronic or terminal illnesses—about the patients’ goals for future care, it can be a vital part of the advance-care planning process. But it’s often awkward to have these conversations, particularly when they are about the end of life, the study said.
“If a patient wants to attend a beloved grandchild’s wedding or travel to a favored destination, treatments that could potentially prevent her from doing so should not be instituted without ensuring her understanding of the life impact of such treatments,” the study said.
Discussing a patient’s bucket list is just a good way to start these conversations, Periyakoil said. Most people are far more open to talking about their life’s goals in this context before filling out an advance directive, a written statement of a person’s wishes regarding medical treatment at the end of life, Periyakoil said.
‘Find out what actually motivates them’
“It’s important for physicians to talk to patients and find out what actually motivates them,” she said. She encourages both doctors and patients to bring up the topic of a bucket list. By discussing how a treatment or surgery might affect the patient’s life, and then discussing what the patient’s goals are, the best possible care plan can be laid out, she said.
“I had a patient with gall bladder cancer,” Periyakoil said. “He was really stressed because he wanted to take his family to Hawaii but had treatment scheduled. He didn’t know he could postpone his treatment by two weeks. When doctors make recommendations, patients often take it as gospel.”
After an informed discussion about his options and the side effects of the cancer treatments, he and his physician decided to postpone the treatment. He made the trip to Hawaii with his family, then returned to start cancer treatments, the study said.
“Patients don’t see the relevance of an advance directive,” said Periyakoil. “They do see the relevance of a bucket list as a way to help them plan ahead for what matters most in their lives.”
Roughly half of all post-9/11 veterans who may need mental health care do not seek it through the Department of Veterans Affairs or in the private sector, according to a recent report by the National Academy of Sciences, Engineering, and Medicine.
Alarmingly, the report also says a significant number of veterans are unaware of the services available to them from the Veterans Health Administration — the VA’s medical arm.
Veterans who need mental health care but haven’t sought VA help cite several reasons, including “that they do not know how to apply for VA mental health care benefits, they are unsure whether they are eligible, or they are unaware that VA offers these benefits,” according to the Congressionally mandated Jan. 31 report.
“I was dismayed to learn how many veterans didn’t know how to access care,” Ralph Bozella, Chairman the of Veterans Affairs and Rehabilitation Commission for The American Legion, told Task & Purpose. “The VA has done a great job advertising their mental healthcare services on the web and via social media.”
But, he added, “At this point, I think the entire veteran community needs to do more to ensure veterans in need link up with the care they require. We all need to play a more active role here.”
To help with that, here’s a list of mental health services the VA provides to recently transitioned veterans.
Are you a combat vet?
Veterans who served in a combat zone can receive medical services — including mental health care — for five years through the VA, beginning the day of their discharge. This isn’t the same as having a service-connected disability rating; instead, think of it as free health insurance. Eligible vets will have free care and medications for any condition that might be related to their service; there’s no enrollment fee or premium, but you do have to cover copayments. This also opens you up to the VA’s CHOICE program, which means you can receive care through a private-sector specialist at the VA’s expense, not yours.
Soon, every transitioning vet can receive a year of mental health care through the VA.
Last month President Donald Trump signed the executive order “Supporting Our Veterans During Their Transition from Uniformed Service to Civilian Life.” It expands VA mental health care services to the 60% of recently separated vets who were previously deemed ineligible — usually because they lack a verified service-connected disability or service in a combat zone. Beginning in March, all transitioning service members with an honorable discharge will be eligible for 12 months of mental health care through the VA. Though the details of the program are still being worked out, veterans will be eligible to receive care at VA facilities — or in the private sector through CHOICE, if a local clinic can’t meet their needs.
Emergency mental health care is available for veterans with OTH discharges.
Though the executive order provides a year of care to many veterans, it doesn’t cover those with “bad paper” discharges — punitive discharges that preclude access to Veteran Affairs benefits, like education and health care. But last March, the VA launched a separate program offering emergency mental health services for veterans with other-than-honorable discharges. Though not all vets with bad paper are eligible, those with an OTH discharge in need of emergency mental health care can receive treatment through the Veterans Health Administration for up to 90 days — inpatient, residential, or outpatient care.
The VA offers much more if you’re enrolled in their system, though.
Veterans who qualify to register with the Veterans Health Administration enjoy a variety of mental health services. These include counseling, therapy, and, often, a treatment plan that includes prescribed medication. The range of coverage is fairly expansive, with experts able to offer support to veterans suffering from post-traumatic stress disorder, anxiety, depression, substance abuse, and stress, among other concerns. Additionally, the VA offers short-term inpatient care for vets suffering from life-threatening mental illness; outpatient care to a psychological rehabilitation and recovery center; video conferencing with a care provider; and residential rehab programs.
If you need immediate help, or just someone to talk to, resources are always available.
For those in need of immediate support, responders with the Veterans Crisis Line can be reached by calling 1-800-273-8255 and pressing 1; via text, by sending a message to 838255; or online. The conversations are confidential and the line is open 24 hours a day, 7 days a week year-round, and the staff is trained to assist veterans of all ages and circumstances.
There is strong consensus that spirituality is an important aspect of care for patients and family caregivers facing serious illness or end of life.[1] Yet, even the most supported palliative care programs struggle with how to best provide spiritual care, given the large caseloads, limited staff, and challenges of the patient population’s ever-increasing diversity of religious and spiritual needs.[2]These issues have become even more significant as palliative care has shifted to the outpatient setting where there may be even fewer resources.
A recent pilot study[3] conducted among 31 patients with advanced cancer evaluated the feasibility and acceptability of chaplain-delivered spiritual care in an outpatient palliative care setting. The investigators used a well-established intervention known as the Spiritual Assessment and Intervention Model (Spiritual-AIM),[4] which is based on the idea that healing happens in relationships and that all humans have three core spiritual needs:
A need for meaning and direction;
A need to feel self-worth and belonging to community; and
A need to love and be loved, including seeking reconciliation for broken relationships when needed.
During three scheduled encounters, chaplains identified the patients’ unmet needs in these three areas and developed plans to meet those needs. In a pre-/post-test design, outcomes were assessed using well-studied tools that measured patient symptoms, spirituality, coping, dignity, depression, and anxiety. From before to after the intervention, increases were seen in several aspects of spiritual well-being, including the subscales for “faith” and “religious coping.”
Viewpoint
Spirituality is a key dimension of quality palliative care, yet palliative care programs need models of care to integrate spiritual care into standard practice. As with all domains of palliative care, there is also a need to generate evidence supporting clinical practice. This study makes an important contribution to the fields of palliative care and spiritual care by testing a model of outpatient spiritual care and including important patient-centered outcomes.
In their discussion, the study authors acknowledge that other variables might have influenced their findings and that some of the tools they used might be measuring psychosocial factors rather than strictly religious or spiritual ones. However, these overlapping constructs are related to purpose, meaning, comfort, and peace-all of which are associated with quality of life, regardless of the patient’s specific faith or belief system.
Chaplains are the spiritual care specialists within interdisciplinary teams, and their contributions, as well as outcomes of their work, have not been well supported or -studied. The Spiritual-AIM intervention has great potential to guide the training of other chaplains and to help achieve a higher level of care for patients and families.
Founded in 1980, Houston Hospice has evolved from an alternative grass roots concept to a leader in hospice care for people of all ages and all walks of life.
Houston's oldest, largest, independent hospice, we are proud to be a 501 (c) (3) organization that is community-based, community-supported and not for profit. This independence allows us to react quickly to community needs and incorporate new innovations in hospice care.
Thanks to the generous, unwavering support of our corporate and private sponsors, we continue to serve Texans from all socio-economic groups irrespective of a person's ethnicity, beliefs or ability to pay.